Heart Failure with Preserved Ejection Fraction (HFpEF)
Considering its prevalence and outcomes, future projections, and lack of effective therapies, Heart Failure with Preserved Ejection Fraction (HFpEF) represent the single largest unmet need in cardiovascular medicine.1 Although EF is preserved and some patients may even have normal LV size, systolic function may be abnormal in HFpEF, including an increase in End-Systolic Elastance (Ees).2,3
Detailed analysis of contractility, relaxation and volumes require methods such as pressure-volume catheters, which show impaired hemodynamic adaptation, including a blunted increase in stroke volume (SV) with increased heart rate in HFpEF.1,4 Definitive, objective evidence of ventricular diastolic dysfunction requires cardiac catheterization to demonstrate an increased LV end-diastolic filling pressure in the presence of a normal or reduced LV end-diastolic volume.2 Exercise testing during hemodynamic assessment may diagnose HFpEF immediately.3,4,5
A significant portion of stable outpatients with dyspnea may have HFpEF, and may have easily been missed using non-invasive testing according a study by Penicka et al. They reported that in the absence of PV measurements, only 25% of the HFpEF patients studied were HFpEF according to the current Echo guidelines, and only 10% showed increased BNP levels.7
As shown in the figures below, per Kawaguchi et al, PV loops can be used to confirm HFpEF showing combined ventricular systolic and arterial stiffening in patients with HFpEF. The high basal Ees limits contractile reserve and induces high energy costs to deliver a given increase in stroke volume.3 The lower loops represent PV loops during rest and preload reduction. During exercise, however, elevated diastolic PV planes and exponentially high LV pressures are apparent for the right-hand image, indicating that HFpEF is present.
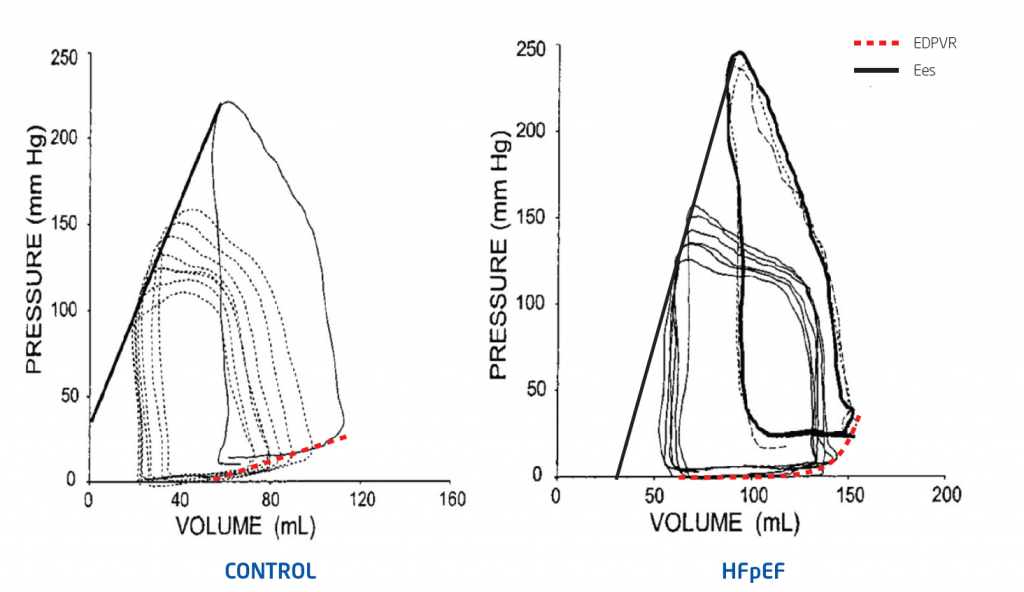
Combined ventricular systolic and arterial stiffening in patients with HF and normal EF (Preload reductions followed by exercise).3
HFpEF Study Highlight
HFpEF as assessed by RV PV loops with handgrip exercise
In compensated stages of the HFpEF syndrome, systolic RV function is preserved, but diastolic abnormalities with intrinsic RV stiffness and prolonged RV relaxation are already present. Impaired diastolic RV reserve contributes to a blunted increase in cardiac output during exertion. Because impairments in diastolic function seem to be a biventricular phenomenon, RV diastolic dysfunction warrants further consideration when characterizing HFpEF patients.8
HFpEF Clinical Trial: DECIPHER HFpEF is a German multi-center study using ventricular pressure-volume loop analysis in 180 patients as reference to validate Cardiovascular Magnetic Resonance and Echo for HFpEF diagnosis. Primary Investigator, Prof E Nagel (University Hospital Frankfurt), started this study in January 2018.9
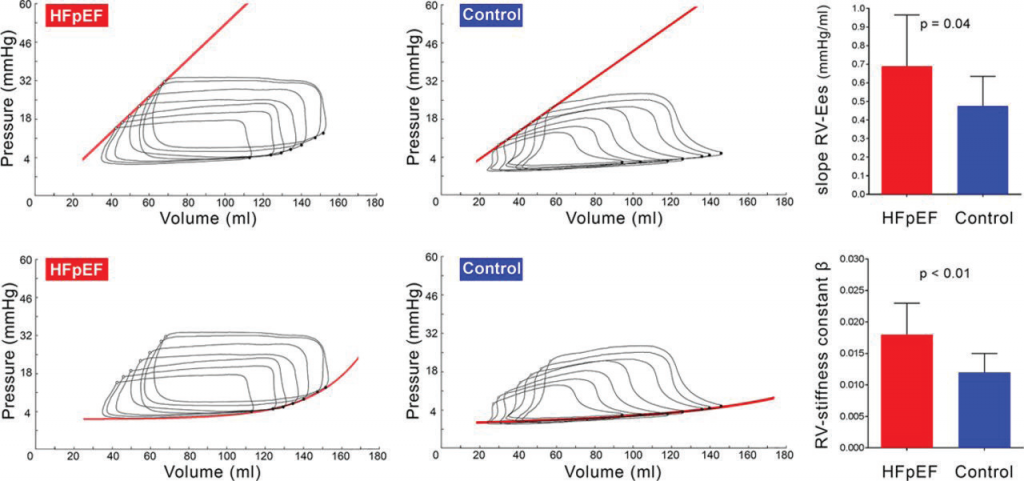
Reduction of preload in heart failure with preserved ejection fraction (HFpEF; left column) and controls (middle column) to determine load-independent markers of contractility (End-systolic elastance (Ees)) and stiffness (ß; right column), in the right ventricle.8
Related publications.
- 2019; Clinical PV Loop Applications: https://academic.oup.com/eurheartj/article/41/12/1286/5552801
- 2018; Load-Independent Systolic and Diastolic RV function in HFpEF: https://pubmed.ncbi.nlm.nih.gov/29449367/
- 2010; HFpEF in outpatients with unexplained dyspnea: a PV loop analysis: https://pubmed.ncbi.nlm.nih.gov/20394874/
- 2009; Invasive Hemodynamic Assessment in Heart Failure: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680766/